Changing the Way We See Behavior
When a child falls apart, screams, refuses to follow directions, or hits, our first instinct as adults is often to stop the behavior as quickly as possible. We build reward charts, offer allowances, or set up timeouts. For a long time, the dominant professional approach has reinforced this: treat behavior like a standalone problem that belongs completely to the child, and focus entirely on making them comply.
But when we step back and look at children through a relationship-focused lens, we see something completely different. Behavior is not just an action; it is a form of communication. It is the visible sign of how a child’s entire body, sensory system, and family relationships are interacting. When a child acts out, they are telling us that their internal coping system is overwhelmed. This guide bridges the gap between everyday parenting and deep clinical understanding, using the brilliant framework developed by Dr. Stanley Greenspan to change how we support children
Two Different Pathways: Individual Problems vs. Family Balance
To understand how to best help a struggling child, it helps to look at the two main ways professionals and families handle behavior:
1. The “Fix the Child” Model (Cognitive Behavioral Therapy (CBT)/ ABA)
This model views behavioral challenges as a missing skill or a bad habit located entirely inside the child. The focus is top-down: teach the child to change their thoughts so they can control their actions. In this setup, parents are often given the role of a referee or a compliance monitor, responsible for tracking rewards and punishments. The subtle message here is that the child is a broken piece of machinery that needs to be repaired. For adults there is some ‘evidence’ that this can help, but children’s brains are different and they don’t have a fully developed prefrontal cortex that would allow them to comprehensively benefit from these behavioral interventions.
The Cognitive Barrier: Over-Reliance on a Developing Mind
The core limitation of applying standard CBT to children lies in its assessment structure. CBT requires identifying “automatic thoughts,” distinguishing complex emotional states, and evaluating cognitive distortions (Halder & Mahato, 2019). Clinical research indicates that:
• Linguistic and Developmental Gaps: A child requires a minimum baseline of cognitive maturity, linguistic competency, and verbal reasoning to benefit from cognitive restructuring (Halder & Mahato, 2019). Children often lack the developmental tenacity to identify abstract thoughts during moments of distress (Halder & Mahato, 2019).
• The Risk of Prompted Compliance: When therapists attempt to guide a child through cognitive discovery, younger clients frequently just adopt the alternative thoughts “suggested” by the adult rather than genuinely processing them (Halder & Mahato, 2019). While this might show a short-term gain in insight, it fails to maintain itself or translate to future, real-world crisis situations (Halder & Mahato, 2019).
Treating Symptoms Instead of the Root Cause
Because younger children struggle to verbalize internal emotional distress, their discomfort is typically expressed outward through externalizing behaviors (such as screaming, non-compliance, or aggression) (Halder & Mahato, 2019). Traditional interventions often make the mistake of focusing strictly on neutralizing these problematic actions rather than addressing the core internal trigger (Halder & Mahato, 2019).
• The Trap of the Token Economy: Operant conditioning methods, such as token economies (TE) that reward positive behavior and penalize negative actions, are highly popular for tracking compliance (Coelho et al., 2015). However, data shows that children who display behavioral struggles rooted in deep emotional regulation issues or a lack of self-monitoring capacity often demonstrate strict resistance and even behavioral deterioration under these rigid systems (Coelho et al., 2015).
• Failure to Cure Underlying Pain: Because behavioral frameworks prioritize present-day symptom management, they fail to resolve deep-rooted emotional issues, complex trauma, or chronic sensory overwhelm. When an intervention relies on suppressing an external symptom without healing the underlying pain, the efficacy of the treatment drops significantly over time, leaving up to half of young clients still meeting the full diagnostic criteria for their disorders post-treatment (Bertie & Hudson, 2021).
Isolating the Child from the Relational Ecosystem
A significant pitfall of traditional models is treating behavioral issues as a localized deficit residing entirely inside the child, ignoring the living ecosystem of the home. Research highlights that a child’s progress is fundamentally bound to the family dynamic:
Isolated Child Model: [Child’s Behavior] ──> Targeted directly via rewards/punishments
Relational Model: [Caregiver Attachment / Stress] <──> [Child’s Regulation System]
• The Impact of Parental Distress: Studies tracking CBT outcomes in youth show that parental psychopathology and high parental distress are robust baseline predictors of treatment failure (Bertie & Hudson, 2021). For instance, a mother’s outward expressions of fear (such as being stiff, tense, or fidgety) or a father’s internal rejection of the child directly contribute to a child’s inability to regulate, rendering standalone child-centered therapy ineffective (Halder & Mahato, 2019).
• Adult Misalignment: When a child is referred for a behavioral consultation, parents are often biased toward stopping the externalized, inconvenient behaviors rather than identifying the child’s emotional distress (Halder & Mahato, 2019). When therapists accommodate this by focusing purely on behavioral management, they miss the important relationships, school dynamics, and home environment that are actively driving the behavior (Halder & Mahato, 2019).
Why a “Bottom-Up” Relationship Focus is Required
Human perception and action operate in a parallel loop of bottom-up sensory data and top-down cognitive knowledge (Shuai & Gong, 2014). However, expecting top-down mental control to override a raw behavioral crisis ignores the biological reality of an overwhelmed nervous system.
When an intervention prioritizes behavior charts and cognitive rules over systemic healing, it leaves the child alone in their chaos. True behavioral resilience cannot be built in isolation; it must be cultivated through parent-inclusive frameworks that focus on co-regulation, family dynamics, and repairing the relational soil in which the child grows.
2. The “Nourish the Relationship” Model (Psychodynamic & Relational Framework)
This approach looks at the child as part of a living ecosystem. A child’s behavior is never just their own—it is a reflection of the shared emotional space between the child, their parents, and their caregivers. A child cannot build emotional control out of thin air; they build it entirely through warm, steady, interactive relationships. If we only target the behavior while ignoring how the family system feels, we miss the heart of the issue.
The Family Dynamic Shift: Behavioral struggles do not mean a child is “bad” or that a parent is “failing.” Instead, they show that the interactive loop between the child’s unique physical nervous system and their relational environment needs closer care, balancing, and support.
The Upside-Down Reality: How Behavior Actually Happens
A major flaw in traditional behavioral plans is the assumption that children think first, feel second, and act third. We tell kids, “Think about your choices,” assuming their brains work from the top down. In reality, during stressful moments, the human brain and nervous system operate completely from the bottom up:
Let’s look closely at how this sequence unfolds in real life:
• Sensory Perception (The Body): First, the child’s body takes in sights, sounds, textures, and movements. If a child’s nervous system is over-sensitive to sound, a simple crowded room can feel physically painful or alarming.
• Emotional Perception (The Heart): Almost simultaneous with a child’s sensory perception, is our emotional perception. If the environment feels physically overwhelming, the child immediately feels a deep sense of fear, anger, or threat. This happens completely beneath conscious thought.
• Behavior (The Action): To cope with that raw emotional state (in our amygdala), the body reacts (Fight, Flight Freeze). The child runs away, screams, or freezes. The behavior is an automatic safety mechanism. This is not a cognitive decision, but instead a deeper emotional reaction a child is unaware of.
• Thought (The Mind): Only after the child feels safe and regulated again can their logic center (prefrontal cortex) turn back on. Expecting a child to “think logically” while they are stuck in a sensory/emotional storm is biologically impossible.
The Learning Tree: Dr. Greenspan’s Framework for Mapping Success
To help parents and professionals visualize this sequence, Dr. Stanley Greenspan created a beautiful diagnostic metaphor called The Learning Tree. Instead of just staring at the behavior (the leaves), this model teaches us to look at the entire tree to find out what is truly happening.
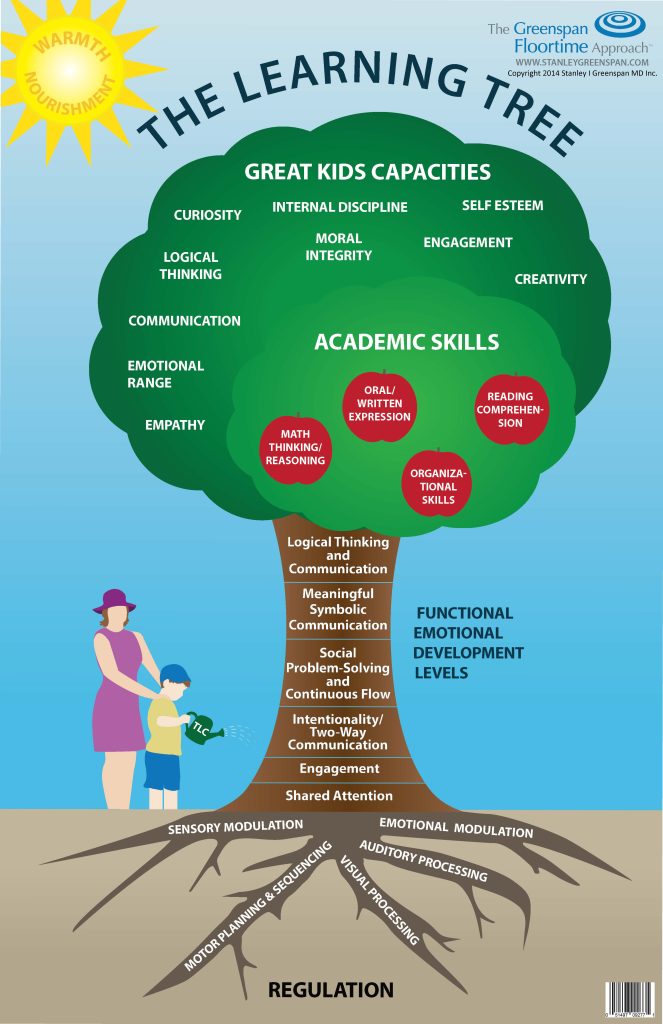
The Leaves & Branches Academic skills (reading, math, writing), behaviors, empathy, and social cooperation. These are the visible outputs. We cannot change them by pulling on them; they only thrive if the rest of the tree is healthy.
The Trunk Functional Emotional Development Milestones (FEDMs). The ability to stay calm, connect with others, communicate intentionally, and solve problems. A sturdy trunk allows a child to handle stress. If a child struggles to communicate their feelings, the trunk becomes weak, and the leaves will begin to drop.
The Roots Regulation (Sensory and Emotional): sensory modulation, auditory processing, visual processing, motor planning, and emotional modulation. This is the foundation. If a child’s roots are fragile or hyper-reactive, it distorts everything that grows above ground.
Looking in the Mirror: Assessing the Adults’ Trees
The most life-changing aspect of Dr. Greenspan’s framework is that it doesn’t apply only to the child. A child’s tree grows directly out of the emotional and sensory soil provided by their parents, teachers, and therapists. To successfully support a child’s growth, we as adults must map our own roots and trunks.
For Caregivers and Parents
Think about your own ‘roots’. If you are naturally sensitive to loud noises (auditory hyper-reactivity) and your child begins to scream, your own root system will register that scream as an immediate physical threat. Your body might instantly move into a fight-or-flight state, causing you to yell back or shut down. When we recognize our own sensory and emotional needs and boundaries, we can consciously work to keep our own roots grounded so we can serve as an emotional anchor for our child.
For Therapists and Professionals
Professionals must explore their own social-emotional trunks. If a therapist has an intense internal need for control or validation, a child’s non-compliance can feel like a professional failure or a personal attack. This can lead to a rigid enforcement of rules that fractures the therapeutic relationship. By mapping our own trees, we learn to share our calm rather than joining the child’s chaos.
Putting It into Action: Greenspan Floortime®
Once we understand the true bottom-up nature of behavior, our daily strategy changes. Dr. Greenspan’s version of Floortime, Greenspan Floortime®, gives parents and professionals a tangible way to put this insight to work. Instead of demanding compliance from above, we get down on the floor, follow the child’s lead, join their play, and gently challenge them up the developmental ladder.
By connecting with the child’s true emotional interests, we help grow their trunk and deepen their roots. When the roots are systematically nourished through warm, attuned, and validating relationships, the behavioral leaves naturally begin to heal, grow, and flourish.
References
• Bertie, L. A., & Hudson, J. L. (2021). CBT for childhood anxiety: Reviewing the state of personalized intervention research. Frontiers in Psychology, 12. https://doi.org/10.3389/fpsyg.2021.722546
• Coelho, L. F., Barbosa, D. L. F., Rizzutti, S., Muszkat, M., Bueno, O. F. A., & Miranda, M. C. (2015). Use of cognitive behavioral therapy and token economy to alleviate dysfunctional behavior in children with attention-deficit hyperactivity disorder. Frontiers in Psychiatry, 6. https://doi.org/10.3389/fpsyt.2015.00167
• Halder, S., & Mahato, A. K. (2019). Cognitive behavior therapy for children and adolescents: Challenges and gaps in practice. Indian Journal of Psychological Medicine, 41(4), 279-283. https://doi.org/10.4103/ijpsym.ijpsym_470_18
• Shuai, L., & Gong, T. (2014). Temporal relation between top-down and bottom-up processing in lexical tone perception. Frontiers in Behavioral Neuroscience, 8. https://doi.org/10.3389/fnbeh.2014.00097
• Greenspan, S. I. (2002). The Learning Tree Framework: Assessing Sensory Roots and Functional Emotional Trunks in Pediatric Intervention. Core Educational Monographs, available at stanleygreenspan.com.
• Greenspan, S. I., & Wieder, S. (2006). Engaging Autism: Using the Floortime Approach to Help Children Relate, Communicate, and Think. Clinical foundations hosted at stanleygreenspan.com.
• Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W. W. Norton & Company.